I live in Trumbull County in Ohio, the dark red county in North East Ohio. We recently had 23 (non-fatal) overdoses in a two-day period[0]. That's roughly .01% of the county's total population - so yeah, it's getting bad here.
There were recently two shootings within a mile of my house. Several people dead. Both shootings were drug related.
I can't help but look around and believe that the needs these folks are trying to satisfy are completely human, and that forcing the users to resort to black markets leads to violence and overdoses. I can't help but think this problem in my community could be solved by simply letting people get high.
Maybe the answer isn't to make heroin available OTC at Walgreens, but supervised injection sites seem to be gaining traction[1]. I think a lot of the dark red spots on the map, like mine, should probably consider this option.
Isn't the counterargument to this to point out the Oxycontin abuse epidemic? Doctors are prescribing years worth of opiates to patients. There have been suggestions that Purdue Pharma's formulation of Oxy practically guarantees dependence, because of the way it's dosed. Are the people dying of heroin overdoses in white rural Ohio starting on heroin, or transitioning to it after prescription opioids become too expensive?
Sam Quinones suggests that the actual trade in Mexican heroin is distinctively less violent than in other drugs; there's a pipeline of supply and distribution designed to be low-key and customer-service driven. If violence is coming from addicts and not from suppliers, increasing supply isn't going to make those people any less desperate or violent.
Checkout Denmark. They had a huge problem with robberies and started giving legal pure Heroin shots to users. They also helped them find jobs. No more deaths and no more black market for Heroin. Hence burglaries also went away.
It looks like our current President is looking at cracking down on pot again though so, I don't imagine we'll have a sensible drug policy anytime soon. Only one motivated by profits.
Which Denmark is this? Doesn't resemble the one I live in. Neither the robberies problem nor the legal pure heroin, and most certainly not the disappearance of burglaries - not statistically, not anecdotally, and not according to the several people of my acquaintance who have had it happen to them.
>Reduced the number of days spent on crimes to a third
Not all crime is committed by heroin addicts so the programs won't stop burglaries completely but they have been shown to dramatically reduce the amount of crimes committed by participants.
I am responding to the "burglaries went away" statement. Nowhere have I claimed that the numbers couldn't have fallen. Your downvote (my assumption) is uncalled for.
That is entirely dependent on interpretation. Taking a comment saying "burglaries went away" at face value to mean ALL burglaries for all causes is just... diametrically opposed to any meaningful debate.
Its obvious that it means drug related burglaries went away, which is a claim we have fairly good evidence to support.
In the USA, there's a fantasy Denmark that exists in the media.
In the fantasy Denmark, there's no crime, all the women are hot blondes who never get fat, there's cheap weed every where (and apparently free clean heroin), the furniture is sleek, all the men are feminists who never objectify women (there's no porn), the school system is fantastic (every child is good at math), the healthcare is free and high-quality, education is universal, free and high quality, and there are plenty of jobs for everyone (and high quality ones too!).
There is a 3 month gurantee. If they have not diagnosed you, and started treatment within that periode, you're free to go to a private clinic or hospital, free of charge.
Yes, but this is a general trentment gurantee. If you get cancer the times have to be shorter, and are shorter usually messured in weeks. It's better but still not good. If there is suspected cancer, you should get diagnosis started the same or next day, and treatment/surgery within a week.
Uhh, hate to break it to ya, but even with insurance its not all roses and sunshine in the USA, you can easily go 6 months waiting for a knee replacement here. Watched a family member go through 4 over the past decade, and its a slow process no matter the insurance provider.
Plus, hospitals here on the West Coast have amped up doing a bunch of skeezy stuff recently, you could easily end up with a non-functional leg at a place like Swedish or Providence (two major hospital systems):
Poor post-op care for the initial two, combined with Stryker making some very low quality knee replacements. Thus why you'd need another knee replacement after a decade
Partially, the upstream vendor (Stryker) made some defective knee replacement joints that wear out prematurely, causing pain and issues walking. Opening the knee back up and replacing most of the parts with better designed parts is what has to be done after a decade, then you get to sit there for months and heal.
Vs in the US where specialists just tell you that your problems are chronic, are pre-existing so not covered by insurance, and that nothing can be done for you.
Both chronic and pre-existing conditions are now covered by insurance.
Granted, a large number of the chronic conditions people face are caused by lifestyle choices and doctors don't have the power to make people want to change how they live their lives.
Not smoking, eating less crap and exercising more would drastically reduce the amount of chronic health conditions Americans face.
High blood pressure, type 2 diabetes, COPD and a host of other problems would drop dramatically if people lived healthier.
Maybe, but I've never heard of someone being told that their treatment is not covered, while in US insurance companies always try to weasel their way out of paying for treatment if they can.
Some supervised injection sites are also able to test the drugs to make sure they're not adulterated in some way that could be harmful. That means fewer trips to the emergency room, less police paperwork, not to mention there's an opportunity to mitigate drug use with therapy and treatment.
Trump should be taken to task for illogical stands, but you're dreaming if you think things would have been better under Hillary. Pharma was paying her to help keep pot illegal. At least Trump is capable of bending since he serves no one but Twitter.
Addicts in The Netherlands get free heroin. Without the daily hustle to find the next high people have time to think instead. A lot of them find the peace to actually quit.
Actually it's really hard to keep the program going as the government doesn't like to be associated with free heroin.
Only very serious cases can get free heroin in The Netherlands. Some of the criteria: you have to be at least 5 years addicted, you need to have tried methadon to get over your addiction first, you need to be a daily user and need to have bad physical or mental health.
None of those people quit after having been admitted to the program. But they do get a better life and are not forced to be criminals anymore.
> Isn't the counterargument to this to point out the Oxycontin abuse epidemic?
I don't see the origins of addiction relevant to arguments about containing current addiction when it moves to the illegal market. But I agree that supply-side targeting when talking about legal industry makes a lot of sense. Being legal, they also have lobbyists, which reduces the impact, same as other legal drug suppliers.
> If violence is coming from addicts and not from suppliers
Others have mentioned this, but opiate abusers don't get violent when high. Some small percentage sometimes get violent when they run out of money to score. Experiments elsewhere suggest that it is a lot cheaper (in money and in human costs) to contain, (in some way) legalize and (if they want it) help them get clean then clean up after them.
I'm not sure I was arguing that opiate addicts are violent when they're high.
I'm not making a moral argument about legalization or even (as is being repeatedly suggested on this thread) subsidization of opiates. I'm saying that if the cause of the epidemic is prescription opioids, and the ultimate problem is "too many people are non-functional opioid addicts", then deregulation won't fix the problem.
> too many people are non-functional opioid addicts
Experience here in Switzerland would suggest that if the state takes dirty needles, expensive supply, and highly variable purity out of the equation, opioid addicts can lead a life that is, while far from ideal, considerably more functional than before.
My impression is that drugs like Heroin, taken in correct dosage, do not inherently cause massive health damage. It's not clear how deregulation would work with drugs like meth, which DOES seem to inherently cause health damage.
by what ROA ? You smoke it, and you're good until your dependence increases. Then you must smoke it to feel normal. But if you slam it, you'll get high again. Do that a while and your dependence increases just as before, now you have to slam it just to feel normal. But if you just got someone to give you their dose, then you could slam 2 doses and get high again...and now you're in overdose territory
If we believe that some addicts can be helped to deal more productively with their addiction (personally I think that's true), and we observe that prohibition tactics don't help addicts get that help (see TFA and basically every other serious examination of this), then ending prohibition will certainly help some addicts. One might argue that more people would start using without prohibition, but that would be pretty lame in the context of the Pill Doctor Pipeline described here.
I understand that it's difficult to avoid litigation of decriminalization (or, apparently, subsidization) in discussions about illegal drugs. I'm generally receptive to decriminalization.
But I'm not making a point about decriminalization. In the same way that it's counterproductive to spend a lot of time talking about prohibition in mass incarceration discussions (significant reduction in incarceration --- which is absolutely necessary --- will require us to adjust sentencing and policies surrounding violent crime among offenders who have never been convicted of drug offenses), spending a lot of time talking about free heroin isn't going to help us if the problem underlying the opiate crisis isn't heroin prohibition, but instead overprescription and negligent formulation of opiate painkillers.
I don't understand this "purity of argument" argument. You'd like to ignore prohibition as a cause of these problems, apparently since this other cause also exists (...conveniently ignoring that they're actually two aspects of the same cause, since pill mills are an unavoidable result of prohibition: never mind that). I contend that looking for "the one true big cause" is a mug's game. Sure, it would be nice if physicians were more skilled at pain management. Maybe they should go back to school? b^) Perhaps if they were more skilled, these problems would be reduced. Regardless, if the prohibition regime changed into more of a treatment regime, that would also reduce the problems associated with addiction, especially for existing addicts who have already received poor care from physicians!
while we're talking about the orthagonality of people's comments, I have one to contribute!
This is the second of your posts I've read in an hour with a b^) (checking your history shows at least one more) and now I'm curious. I've never seen that face before. The first time, I assumed it was a carelessly-executed B^) "2cool4you sunglasses wearer grinning sarcastically," but I guess it's not. My best guess is that it's winking - but winking is usually light-hearted and seems odd paired with the ^) nose/mouth that I associate with black comedy/sarcasm.
If ^) is light-hearted to you, I'd guess "quirky, almost flirtatious wink and grin." If it's not, I'd guess "smirking, exaggerated and heavily ironic wink." For people I know well, I could probably tell which one they meant; for strangers on the internet, less so. Is either interpretation close to the mark?
My right eye is missing and I normally wear a patch over that socket. I've used that smiley for decades; my offline friends usually get it but it's understandable that that someone who's never met me would be uncertain...
Are prescription opiate users as likely to overdose as heroin users? My understanding is that they are not. If you're buying oxycontin at CVS, you're getting oxycontin in the dosage prescribed. At least once a year in Chicago we see a news story about dozens of people hospitalized after using what they bought as heroin but which was not.
Making heroin available to those who want or need to use it may reduce deaths or even hospitalizations without changing the number of opiate users.
> "too many people are non-functional opioid addicts"
Part of the issue with things like heroin is that unlike many weaker drugs the highs are brief. Heroin addicts are as a result very often highly functioning if they don't have to worry about where to get their next high and can get highly consistent doses.
I worked with one years ago, and we only realised when a series of large busts drove prices through the roof and he started spending his time looking really nervous and on the phone until suddenly disappearing for two days once prices normalised and he "made up" for the stress by staying high most of those two days before checking himself into a hospital (which was when we finally found out). He was married and had kids, and neither his family or his co-workers had noticed a thing through years of addiction prior to that, despite having to struggle with an illegal supply.
There are lots of problems with heroin, but many of the worst ones are a direct result of addicts inability to meet their needs in a quick and "safe" way.
I'm not sure "epidemic" is a good word here. When compared with infectious diseases, we see that cause (the microbe) and effect (from fever to death) are clearly related. Here we have deaths caused by a prescription. Why were opioids prescribed to start with? And if abused, why?
The problem with Oxycontin is that it's supposed to have a twelve hour window of action and doesn't. Doctors prescribe larger doses rather than more frequent ones because that's what the label says. That's the language the FDA approved. Repeated cycles of high dosage wearing off a few hours too early is a bad thing, builds up more tolerance than consistency.
The cost of medical grade heroin is a tiny fraction of the costs to society of the crimes to support illegal heroin.
So if the issue is money, then the case is even more strongly in favour of legalisation.
We don't even need to give it away for free - just giving addicts the opportunity of buying medical grade heroin at cost would massively improve things.
Even better: Heroin addicts can generally function relatively well when they don't have to chase their next high constantly. Giving them a secure supply would let many of them hold down jobs and pay taxes and cover their own costs.
The economics are all in favour of shutting down the "war on drugs" for all but the very worst drugs. Incidentally, though, most of the truly nasty drugs are not drugs people tend to want, but synthetics introduced to circumvent drug laws. Most of them will largely have demand evaporate overnight if people could legally get safer alternatives.
Whenever this comes up it's important to realize how much addicts are already costing us. It's hard to know exactly how much because the costs are born by already existing systems - home insurance to cover burglaries, auto insurance to cover smash and grabs, law enforcement to investigate these crimes committed to feed addictions and to try to stop the flow of heroin.
Then there is the cost of health care. Even if you ignore long term problems like HIV or Hep-C infections contracted by sharing needles (hundreds of thousands of dollars per person), just responding to overdoses is very expensive. [0]
>In December 2016, the City of Vancouver approved a small property tax hike, which was intended to help address the opioid overdose crisis. Councillors passed a budget that included a 0.5 per cent property-tax increase to support front-line service providers, which is in addition to the 3.4 per cent increase already in place to deal with the fentanyl crisis.
>..
>According to the report, the total funds available in the 2017 contingency fund for the opioid crisis is $3.5 million and the remaining amount after the above expenditures is $1.4 million.
That is only the monetary cost, there is a mental cost as well. [1]
>A health and safety worker with Vancouver Fire and Rescue Services says he's never seen stress and anxiety so rampant among first responders.
>Acting captain of occupational health and safety Steve Fraser says the ongoing overdose crisis has many firefighters dealing with emotional and mental fallout because of their job.
>...
>Another big issue, Fraser says, is "compassion fatigue" which comes from sometimes treating the same people time after time.
>"It's that feeling of helplessness and hopelessness that what you do is not making a difference," he said. "For all of us … why we do it is we do want to make a difference. So, when we see that fail time and time again it does start to take its toll."
Heroin clinics would help solve most of these issues. [2]
>Crime Issues: 60% drop in felony crimes by patients (80% drop after one year in the program). 82% drop in patients selling heroin.
>Death Rates: No one has died from a heroin overdose since the inception of the program. The heroin used is inspected for purity and strength by technicians.
>*Disease Rates: New infections of Hepatitis and HIV have been reduced for patients in the program.
>Note: The Swiss save about 38 dollars per day per patient mostly in lowered costs for court and police time, due to less crime committed by the patients.
Identifying the source of the problem is easy, though. Solving the problem for the masses who already find themselves in the midst of an addiction they might not even know they're in yet is much harder and what places like these injection sites are aimed to address.
I believe most of the deaths are a result of the prescription decline. As the DEA and Florida shut down Oxycontin users were forced to turn to the cheaper more available heroin. Evil cartel members mix Fentanyl in Heroin to make profit and they are killing users (their customers) left and right.
They're down barely double-digit percentages from all-time highs. It's a hopeful trend, but not one that rebuts the role of pharmaceutical opioids in the epidemic.
> Are the people dying of heroin overdoses in white rural Ohio starting on heroin
A minor nit, but how many people are overdosing on actual heroin, and how many on eg fentanyl?
> If violence is coming from addicts and not from suppliers, increasing supply isn't going to make those people any less desperate or violent.
The argument is something like: If there's a limited supply the price increases and people turn to crime to get the money. If there's a government supply as part of addiction treatment (and a package of other care) there's reduced need to find funds.
Here in Canada heroin is also associated with less violence since its relatively inexpensive from the source so losing a load from India to customs isn't the end of the world to a drug dealer's operation whereas cocaine is traded on large loans, so any loss means violence is the only answer to get the money back.
What's happened the last few years is even cheaper synthetic opioids is available from Chinese factories, and as it's legal there no connections are needed to export it, so mid-tier and lower street gangs here have made their own startups buying and exporting the cheap synthetics (Fentanyl, Carfentanil ect) directly effectively bypassing the traditional pipeline that was bringing in heroin for decades. Naturally this has lead to a ton of violence and overdoses as users get synthetic adulterated heroin instead of their usual dose and gangs fight over control of the much more profitable synthetic trade.
When China and other countries makes the synthetics illegal (China already made it illegal to export to Canada a few weeks ago, not sure about the US) it will go back to being too expensive to self import since petty gangs here will need connections there, and the heroin pipeline will resume again with overdoses falling until of course, another loophole legal synthetic is discovered.
That's not really a counterargument. Sure, Purdue and other opiate pushers got people addicted, and tweaked distribution to get around regulation. Then governments freaked, and locked down prescription opiates. So addicts have turned to heroin. But they're naive about heroin, so they tend to fuck up and overdose. And then there's the problem that dealers boost unpredictably with Fentanyl. And about user violence, you don't want hungry junkies around. They will do whatever it takes.
Why not pull a Denmark, legalize and give at no cost heroin to addicts, and get these people back to work? A junkie can be productive, despite an ongoing chemical addiction, whether it be meth, heroin, alcohol or whatever else, many middle class and upper class folks live productive lives despite these addictions.
Why can't we bring these people back into being productive, economically net positive members of society, and deal with their addictions with compassion, as any reasonable human being & the Catholic Church preaches?
I've employed many addicts before, if they have a choice of smashing windows all night to maybe get $100 worth of shit they'll fence for $60, or a gig that'll pay them $110 to pull cabling & set up hardware for 8 hours, they will pick the latter every time. Outside of work hours, don't expect them to be contactable, and watch your shit well, but beyond that this group of humans can be a net positive for our society despite the chemical dependency issues they have.
I think Denmark decriminalized heroin, but didn't legalize it. The distinction being that an addict is no longer a criminal, so they can get treatment without fear.
But the original access helps feed the epidemic. You don't become an addict until you do, right?
Tobacco is as addictive as heroin[0], think about how much of a public health issue smoking has been. Do you think it would be that if tobacco was illegal? I could imagine making heroin legal would create many more addicts.
One of the core arguments for marijuana restriction is that it's not nearly as addictive as "hard" drugs. it's comparable to things like alcohol.
Access restriction seems like a good idea when a substance is so addictive that you develop lifelong dependence from it by default.
Tobacco is far more addictive than opiates. And health and societal impacts are far worse. With consistent and affordable supply, opiate addicts can lead otherwise normal lives. No worse than caffeine addicts, really. And if there's chronic pain that's otherwise untreatable, the fact that they're addicts is almost irrelevant.
You mean less violent within the U.S., right? Because believe me that keeping drug prohibition in the U.S. and the bilateral consensus of fighting drug trade militarily is causing quite a violent situation in Mexico, to the tune of 200,000+ dead by official numbers in the last 10 years (>0.2% of national population, and arguably the official numbers are a severe under-estimate).
In fact, it is, because if the pathway to addiction starts with overprescription, deregulation is unlikely to alter the stats: prohibition and black markets aren't gating factors.
I think we'd need more evidence of that before just assuming it. Some number of people with current addictions would not have developed a habit if they hadn't been supplied by their doctor. Sure, there are also folks out there with habits that "doctor shopped" or whatever, but we aren't talking about those.
Now, if "deregulation" as used above means "stocking next to aspirin at CVS", then sure. But that's not what's being discussed. Haven't done a study of it, but I'm pretty sure Denmark doesn't have many folks heading signing up as addicts to experiment.
You need to capture not just addicts who got started on prescriptions, but addicts who got started through the resale of overprescribed opiates from non-addicts.
Also, the demand from Oxy addicts created (or, I suppose, upgraded) a criminal network that supplies heroin. When I was growing up there weren't that many heroin addicts around, so the local independent pharmacies didn't stock it.
If you were an adventurous youth looking for a new high you would have been sold barbiturates, maybe, or benzodiazepines. Maybe speed. But today it would be heroin, and you can trace at least some of that back to oxy addicts desperate to feed their addiction after being cut off.
What is? You didn't actually argue anything. I have no idea what you're talking about. Pointing out that Oxycontin is being abused is not an argument. What is your position?
Even in the US heroin use was massively down, because it had moved on from the edgy rock and roll era to realising how dangerous it was. The list of dead celebrities rather took the edge off heroin chic.
The US resurgence is tied to massive over-prescription of opiates who abusers turn to heroin if their supply is disrupted / their tolerance increases. The demographics of users is very different. There's an entire chapter in Narconomics covered to this. Supervised injections etc works in Denmark because its healthcare sector is set up to support it - the US healthcare sector is still actively poisoning the populace.
Given the amount of pharmacetical money sloshing around every single congresspeople's coffers there will not be any meaningful reform or restrictions for a long while. The easiest path is to just go full-bore law and order against drug users.
I think people are taking away the wrong message here. It's the "easiest" as in "on the lowest shelf". It's easy just as it's easy to grab undocumented immigrant parents in pickup lanes at schools.
There's doing what's hard (either politically, or by effort) but "best", and there's being lazy and incompetent and just doing what comes easiest. Our current administration does the latter.
If there's more crime, that means you can shout louder about law and order next election cycle. It doesn't matter that the crime was your fault and that you're going to make it worse. What matters is that you buy the police more guns and shake hands with local police chiefs a lot.
i have a friend (in the US) who used kratom to kick heroin. he still has an addiction to service but it's legal, relatively cheap and not debilitating. i know he's not alone in this use of it, though it's also a useful anxiolytic ime, and i had no issues with addiction or withdrawal after experimenting with it a little.
i was very hopeful about the obama dea backing off the kratom ban last autumn after the public backlash but i'm worried about steps the current administration may take.
They're not legal in The Netherlands. Magic mushrooms have been banned a while ago (but at the same truffles still are not, clueless), weed was never legal. Also all production is illegal. Coffeeshops don't pay taxes.
They're just.....there?
We used to think it was the crazy US forcing the Dutch to have such a bipolar approach to drugs but pot is more legal in Colorado now than in Holland and still the Dutch laws are a mess.
Magic truffles have the same effects as magic mushrooms and are legal. Magic mushroom products are still sold at some smartshops, but not legal. Weed is not legal, but you can buy it in dispensaries ("koffieshops") and carry up to 5 grams without being fined or arrested. You can smoke publicly as long as you're not bothering anyone (like with alcohol). I think that's pretty sweet.
You can have up to 5 plants at your home, but if the police asks you to destroy them you have to, or you can get fined, so again: as long as you're not bothering anyone or dealing you're fine.
There are is also a proposed law to decriminalize the mass-production of weed (while introducing QC regulations, like those for food) and the delivery to the dispensaries.
With that full legalization can't be far off. The idea that legalization is just the right thing to do is pretty mainstream here, and a progressive political party, GroenLinks, supports legalization and is currently 3rd in the polls.
I think that's an urban myth actually. I know people that got kicked out of their house for having just three plants just growing outdoor so no tampering with electricity or fire risk. They used to be more lenient but people tended to burn their house down with illegal indoor plantations.
It's weird how in a liberal country like The Netherlands where everybody wants full legalization we somehow ended up with a government that got a lot stricter instead.
So you can't have any plants at all but if you have more than five you will always be persecuted. Perhaps the renter that got kicked out had violated some kind of agreement. It was social housing though, which is really common in The Netherlands, so I imagine a lot of people are facing the same problem.
Yeah, but why would the police ever see your plants at all?
Also keep in mind that the police in the Netherlands is not as trigger happy as American police by a long shot. You're not getting swatted for having a few plants because our police is not militarized at all, we have a separate branch of LE that does riots and SWAT-like tasks and they're mostly used for large drug operations and soccer riots.
AFAIK as long as you're not using high-powered lighting (and not the modern LEDs or sunlight), tapping the neighbors' electricity and therewith creating a fire hazard you're fine.
Plantations are usually found either by the electricity company or because a helicopter with IR vision (or regylar vision on a snowy day) happens to find a house with an unusually hot roof.
The legal status IMO is less important in this case than how the state treats it. In the Netherlands (correct me if I'm wrong), drugs are seen as a public health concern, and in the US its seen as a criminal problem. When its criminalized and demonized like it is here, then politicans must "crack down" on it to appear "tough on crime", and more progressive mitigation solutions (like supervised injection and treatment centers) aren't even entertained in our lust to imprison.
My understanding is that the reintroduction of prescription opioids is a major source of new addicts. Once the prescription lapses, people have often become addicted and seek out other sources.
It's clear that we need to do a lot more to help these problems, as you suggest. We can also do a lot to keep people from getting addicted in the first place, by choosing (and regulating) better options for pain relief.
You may be interested in Portugal's drug policy which has become an example of what you're suggesting. Laws were relaxed in 2001 together with increased support and therapy. Statistics suggest that drug use and related problems have reduced since then:
https://en.wikipedia.org/wiki/Drug_policy_of_Portugal
> Maybe the answer isn't to make heroin available OTC at Walgreens
Actually, in UK you can get actual opioids (as co-codamol) behind the counter, without a prescription. Funny how they don't seem to have a disastrous and deadly opioid epidemic like the US has.
I'd so much rather live where people can get cheap pharmaceutical grade heroin at the pharmacy than where people who need opioids end up smashing windows to steal my laptop to buy some dangerous and overpriced fentanyl contaminated "heroin" that ends up making them overdose in the street (transnational criminal organisations tend to lack purity standards commensurate with those of prescription drug manufacturers, weirdly enough).
Crackdowns on "pill mills" and "doctors who overprescribe" is what denies people a safe and legal source of pharmaceutical-grade opioids and forces them onto the black market of illegal, extremely overpriced, dose-uncertain, and fentanyl-contaminated opioids -- all of which make drug use a lot more problematic and dangerous (for both the user and the community) and pushes people from "drug dependence" (needing a regular, constant dose of a medication to function) to "drug addiction" (problematic, damage-causing drug use).
Dose uncertainty especially contributes to the harm of drug use -- if the doses aren't uncertain (and are precisely metered like those of other, pharmaceutical-grade medications), it's a lot easier for the user to find the right dose that extinguishes the withdrawal symptoms and the pain while not ending up anywhere near an overdose. Also the ability to access pure opioids with precise doses means it's a lot easier to take the drugs as a periodic, regular dose and not have one's life disrupted by extreme highs and extreme lows and drug-craving. This allows users to maintain a normal, productive, non-criminal life with other things in their life (family, hobbies, career) than just the pursuit of opioids.
In US, the "epidemic" of OD deaths only began when crackdowns intensified on legal, pharmaceutical, sources and prescribers of opioids. The DEA cracking skulls over opioids and investigating doctors is literally the only reason illicit fentanyl (and its even nastier analogues) are common illicit products now. I am so very doubtful that skull-cracking and door-kicking will miraculously work after decades of it not working. Prohibition has given us carfentanil in illicit heroin. If you don't know what that is, it's a fentanyl analogue so potent that it's been successfully used as a chemical weapon. This is not an anomaly -- it's just the "iron law of prohibition (https://en.wikipedia.org/wiki/Iron_law_of_prohibition) at work.
> It's not like anything else is working.
Prohibition isn't working, and has caused tremendous devastation to society, and the opioid epidemic is just another instance of this. Prohibition has to get wound down, from the top (end the Single Convention on Narcotic Drugs and the statutes that give it effect) to the bottom (make it so local police can't arrest or search people for any drugs offences (possession, manufacture, use, transport, sale, purchase) regardless of the drug or quantity).
> Actually, in UK you can get actual
> opioids (as co-codamol) behind the
> counter, without a prescription.
> Funny how they don't seem to have a
> disastrous and deadly opioid epidemic
> like the US has.
Cocodamol is 8mg of codeine to 500mg of paracetemol. To get 240mg of codeine -- equivalent to 10mg of oral oxycodone -- you'd need to take 30 cocodamol pills, which is 15g of paracetemol. If you present at a hospital having taken more than 12g, they'll put you on a acetylcysteine IV (and generally assume you were trying to end your life).
Actually, in UK you can get actual opioids (as co-codamol) behind the counter, without a prescription. Funny how they don't seem to have a disastrous and deadly opioid epidemic like the US has.
Because it is sold over the counter, buyers have to first talk to a pharmacist to get it. This will likely involve discussing what you're suffering from, so that the assistant is sure that what you're buying is appropriate. Finally, they aren't going to sell you ten packets of pills at once, you'll get just one pack containing a few pills.
So, to get an addict's amount of codeine, you're going to have to visit all the pharmacies in town and give each of them a story about terrible dental pain or some such rubbish. It's just not going to be practical.
My sister is a heroin addict. To say this has devastated her life is an understatement. Her body is wrecked. She looks way older than she is, she has a pacemaker / defibrillator installed in her chest. And doctors keep saying she will die soon if she doesn't stop.
Here is the most frustrating part. She has wanted to go to rehab a few times, but since she is poor and unemployed, she has no health insurance for rehab. What are her options? My parents have no money to help her.
I'll never understand the bull-shit US policy towards drugs. Let's spend billions upon billions to "fight" drugs coming into the country, but let's turn a blind eye to the companies pumping out hundreds of millions of pills.
Why the hell don't we spend those hundreds of billions on actually treating the disease? If there was no demand, there would be no drug war to fight. Why don't we try a new way?
I became a heroin addict at 16. I got clean, for free, with my governments help (Queensland, Australia) and opiate replacement therapy, after being an addict for six years. Ive been sober for 5 years this August. If it wasn't for that program, I'd be dead twice over by now, I'm sure of it. I'm sorry about your sister, it's horrible :(
An idea to help with this would be to call your senator/congressperson and ask that mental health and drug rehab be added to affordable care act. I'm not sure if that type of coverage is there but if they can get it added to the revamped legislation then maybe people in your sisters situation would have some avenue of hope.
For their chemical makeover, the researchers noted that when tissue is damaged and hurting, it becomes inflamed and more acidic. The pH drops from approximately 7.4—what’s seen in normal, healthy tissue—to between 5 and 7. Fentanyl can work regardless of the pH, so it’s active throughout the nervous system no matter what. But, if it was altered to only work at the lower pH, then it could target just the pain source at the peripheral nerves, the researchers hypothesized. And with no activity in the central nervous system, it would dodge opioid’s serious side-effects, including addiction and systemic responses that can be lethal during overdoses.
They're testing a modified version of fentanyl that only works in lower pH, restricting its activity to injured areas of the body, eliminating the risk of overdose and dependence:
In further experiments, the researchers noted that, unlike fentanyl, high doses of NFEPP weren’t lethal to the rats. And rats on the NFEPP didn’t display impaired motor activity or reward-seeking behavior linked to addiction.
That's great, and there are other painkillers on the horizon too, but that's "maybe" and "later". Today we could take concrete steps to alleviate this crisis which we created in the first place. Cannabis is a good choice for people addicted to opiates, along with medical detox. You also have to manage underlying mental health, social, and medical issues.
No amount of throwing new molecules at these problems will solve them.
But, if it was altered to only work at the lower pH, then it could target just the pain source at the peripheral nerves, the researchers hypothesized.
It's been a while since I took a pharmacology class, but opioids work centrally - that is, the pain relief is due to their action in the brain. That's why an opioid like loperamide (can't cross the CNS barrier) doesn't have an analgesic effect, only constipating.
If fentanyl only worked peripherally, it wouldn't have a painkilling effect.
Opioids act by binding to opioid receptors, which are found principally in the central and peripheral nervous system and the gastrointestinal tract.
Recent investigations discovered opioid receptors on peripheral sensory neurons.A significant fraction (up to 60%) of opioid analgesia can be mediated by such peripheral opioid receptors, particularly in inflammatory conditions such as arthritis, traumatic or surgical pain. Inflammatory pain is also blunted by endogenous opioid peptides activating peripheral opioid receptors.
Thanks for digging up the references. My only thought is there is evidence that the peripheral effect is either weak or non-existent. Loperamide is a great example. mu-opioid agonist that doesn't penetrate the brain-blood barrier. Will constipate you (by acting on GI opioid receptors), but has no analgesic effect.
> But, if it was altered to only work at the lower pH, then it could target just the pain source at the peripheral nerves, the researchers hypothesized.
Do you know how this interacts with anti-inflammatory drugs?
Given that this article only touches on the supply of these drugs, is there a tacit assumption that the demand for opioids is driven by unemployment? If so, what can be done about the demand for these drugs in the long term? "Bringing back jobs" to those people whose comparative advantage is no longer manufacturing by taxing robots or imposing tariffs is a temporary stall, and to the degree it does work it amounts to a fat, inefficient handout.
Fighting the "epidemic" at the supply level seems like a losing battle, as it is for the hard drugs that plague inner cities. Addressing it at the demand level has to be the answer, but I don't see any possible answers floated.
I think its more dissatisfaction with life in general, with unemployment maybe being one of many triggers.
You're probably right about addressing at the demand level. But, I see the problem being more societal - think no one really understands everything. You take away self-reliance of people (whether they realize it or not) at many levels... its cheaper to get some good-enough quality food at 13 places near my home, so why should I learn to cook. I can get any vegetable I want at the store, so I probably don't need to learn how to tend a garden. In both instances as examples I'm losing a little control of my life. And then....
TV gives me entertainment, and the internet even more so, so maybe i'll just sit back and let it entertain me. So maybe I don't need to read anymore. Its easier to have short non-contextual entertainment bits, which rewire my brain further to think differently [wrongly?]... [0]
And, now capitalism has made all margins of businesses so slim that there's no real way to enter a business and still have a safety net in case you fail. You either need to disrupt an industry, create a marketplace, find a niche, or fail hard.
I think we're just starting to see the uglier stuff here. Short of some great awakening I also don't see the correct prescription. Pun intended.
Postman's book is now 32 years old! I read it as a teenager, which dates me...
I'm not sure about the Amusing Ourselves To Death stuff or the tut-tutting about cooking and gardening, but overall, though, I think you're on the right track. I'm sure that between automation of both manufacturing and services, big-box retailers and the fact that the covering of the 'long tail' is done very well by web-based business. It's hard to picture what a lot of people are going to be able to do in this circumstance and there seems to be the real potential for a cascading unpleasantness.
If you even half-believe the 'technological unemployment' worry, the scary part is that the non-automatable jobs that involved providing goods and services to those displaced by technology will also suffer.
There may be plenty of spare time for people to have that 'great awakening', whatever that might turn out to be.
two examples of many, admittedly probably too personal. Others: technology obsolescence, and the move toward not actually OWNing anything so nothing to learn to repair.
>>If you even half-believe the 'technological unemployment' worry, the scary part is that the non-automatable jobs that involved providing goods and services to those displaced by technology will also suffer.
Yes... My context is now that as a parent, I'm seeing windows closing for the kids' future that I had. I mean programming (maybe; I hope) and robot repair will be very lucrative. So will professions like plumbing and electricians.
I feel the 'parent context' too. I have kids old enough to be thinking more seriously about what they want to do when they group up (i.e. early teens) and it's difficult to know what to tell them. I suspect that many of the hopefully lucrative paths you mentioned will be things that gets more and more 'sealed' and routinized (i.e. robot repair == "remove broken assembly, put in new assembly, send broken assembly to factory in low-cost geo for salvage/repair").
It's not all doom and gloom, of course, and I think it's important to maintain a positive outlook esp. in front of one's kids when talking about this stuff. And of course, the growing helplessness and screen addiction of many of their peers suggests that in competitive terms, finding and holding a good job might be easier and easier (which isn't very encouraging overall, but appeals to the "amoral familism" streak I occasionally get).
> And, now capitalism has made all margins of businesses so slim that there's no real way to enter a business and still have a safety net in case you fail. You either need to disrupt an industry, create a marketplace, find a niche, or fail hard.
While this is true, phrasing it like a critique of capitalism seems very, very weird. As if in a socialist or communist society starting a business is supposed to be easier and margins larger. (Disclaimer: I have founded two failed startups to date, still living on friends' couch after the second one now).
Fair enough, I think I mean distribution of wealth. Capitalism is VERY good at moving money up. But, lately, in America, there's been not enough ways to get money going back down.
You're phrasing it as if you're comparing it with something. Have you ever lived in a communist country? I have yet to see a "redistribution of wealth" system that actually distributes more wealth than it lives for itself.
> Seems like attacking the supply is great place to start.
That is what was done, transferring the demand to heroin as opposed to oxy. Also, focusing on the supply side of things is the last 30 years of US policy: it's not worked effectively, and has a concomitant effect of incentivizing black market dealers to be wealthy and power. It'd be better to sell OTC heroin than to fund violent gangs, just in the name of limiting side effects.
Pills were given out like candy, then restricted which caused demand for cheaper alternatives. Had the drug companies been regulated in the first place, we might be OK.
The pills aren't coming from mules or cartels, they are coming from US companies. The pill supply has to lowered.
However now the US made that mistake, what's the problem with continuing to give out the pills "like candy", although with tighter controls to make sure that they don't go to create new addicts?
For people with short term pain, or who are at the end of life, opioids can be a good choice.
For people with long term pain opioids can, rarely, be a good choice, if other things have been tried first, and if there's a careful package of care.
Most people with long term pain need variations of / combinations of:
1) Access to evidence based pain management specialist clinics
2) Graded strength building exercise (for musculo-skeletal, not for nerve)
3) Medication that isn't opioids
Giving opioids to people with long term pain isn't a good way of controlling their pain (they develop a tolerance) and risks severe harm (on top of addiction).
Here's a website from the English Faculty of Pain Medicine, which is part of the Royal College of Anaesthetists. They explain it far better than I can.
I'm not sure if this is inherent in your #1, but there should be an increased focus on alternative methods for dealing with pain. For instance, since starting meditation training, I haven't needed so much as a single Ibuprofen. It's not that my incidence of pain has decreased, but my way of thinking about/reacting to that pain has changed dramatically and I can now make just about any pain quickly fade into the background. It's also helped me to clarify the difference between pain and injury to know when I can push through the pain and when I need to pull back and rest.
I learned an important lesson, however. Doctors will frequently use the amount of pain someone is experiencing as a diagnostic aid when determining a patient's diagnosis. I had a ruptured eardrum that I saw a doctor for and that doctor misdiagnosed it because I wasn't showing any signs of pain and that injury is supposed to be excruciating. The doctor explained to me that if it was ruptured, I'd be near tears and screaming for pain medication.
Yes, I agree. Whenever I've mentioned cognitive behaviour therapy for pain control, or meditation for pain control, it derailed conversation into discussion about pain that was "real" or "all in the head", with some people refusing to see that in some cases there's no difference: the patient is in real pain, the pain is debilitating, and the treatment has a psychological component.
some possibly sunny news: experiments with a new fentanyl-derived opioid that acts only as a local analgesic and doesn't cross into the brain, meaning no high, non-addictive, and one can't overdose. this is very preliminary (rat experiments) but i'm hopeful:
They don't need to be given out like candy. That's the point. The supply needs to be drastically reduced to prevent new addicts and we should be looking at what other countries are doing for their existing addicts: safe injection sites etc.
> Had the drug companies been regulated in the first place, we might be OK.
What are you talking about? Everything in medicine is highly regulated. Introducing a new drug is a very expensive process, run in the US by the FDA. It takes all sorts of expensive tests and trials to be allowed to sell a new medicine in the US.
Maybe the process messed up in this case. Sure. Many things are possible. But this was regulated start to finish.
MD's are often compensated based on patient assessments. "Rate your doctor" sort of things. How do you think opioid addicts rate doctors who tell them they have had enough?
I agree with the substance of your comment - opioid over-prescription is a huge problem.
The stat though about Kermit, West Virginia example has to be due to fraud and illegal sales, though? Or include vastly more people within the area covered by its pharmacies and/or doctors, which ever the data source used?
Otherwise each person in that town is receiving (on average) 31 pills/day. Maybe I wildly misunderstand hydrocodone prescriptions, but dozens of pills per day seems to be an excess.
I agree that opioid over-prescription is an issue, but I imagine some of these numbers are being inflated by similar "pill mills" run by unscrupulous doctors.
We have the numbers because the DEA tracks it. Why they didn't look into the numbers is beyond me.
Manufacturer seems to have played a role too by sticking to dosing they knew was ineffective and then pushing for higher doses which lead to big bonuses: http://www.latimes.com/projects/oxycontin-part1/
[Apologize for the back-to-back EconTalk plugs, but I really enjoy the show!]
This EconTalk episode on Narconomics goes into a great deal of detail regarding exactly how structurally broken the supply-side attacks are; I found it quite fascinating!
The root cause was the never-allow-pain mantra of the 90s when it came to proscribing painkillers like Oxy; this was followed years later by a later tightening of prescription policy that led many to look to Heroin as an alternative.
You have to understand the context of what you call "the never-allow-pain mantra". The drug warriors had gotten us to the point where you couldn't get treatment for pain. Doctors were harassed out of prescribing opiates and would give you Tylenol for back surgery. People in hospice were allowed to spend their final days in terrible pain.
And now we're heading back in that direction. For some reason we can't seem to stop in the middle somewhere.
> For some reason we can't seem to stop in the middle somewhere.
After observing this country 20+ years I have concluded that extremes rule. Nothing ever ends up done via a measured and calculated approach, always extremes. You can see that in politics, economic distributions, rules and lack of there of (deregulation). It's not just today; I've been reading a fair amount of history and it's like in the DNA of the country.
The resulting crackdown did exactly what you said, drove people straight into the open arms of heroin.
Tightening the already tightened restrictions would only worsen the issue.
Diversion, etc cannot be stopped and you might just see a sudden uptick in pharmacy truck heists like the one that happened five or so years ago. Corrupt pharmacists unable to resist the temptation of easy money, etc.
Or worse, heroin continues to spread like wildfire. Heroin has no QC, it's being cut with fentanyl across the country and addicts are dropping like flies. Sicker addicts have been seeking out these OD stories and score from those areas looking for the fentanyl cut H. It's bad and only getting worse, as if the government overcorrected its steering and has now spun out of control. The result is going to be a grisly accident.
I just go laparoscopic surgery. I told them multiple times I didn't want to use opiates to manage pain, that I wasn't in very much pain, and they still gave me iv fentanyl, and about 150 Vicodin tablets to take home. They asked me if I had an opiate problem, like turning down opiates meant that I had some kind of drug issue. It was bizarre.
I've had Vicodin prescribed a couple of times. I never felt it did much. Certainly didn't make me high. I don't see how it's a gateway to opioid addicion unless you're eating them like candy from the get-go.
I can't believe that many more people, especially (and coincidentally?) in the inner cities, need pain meds. This seems like something bigger in my mind. But I also don't have any data to back it up.
> This doesn't help the root cause of people starting to use them in the first place.
I don't think you can stop at drug use and claim "root cause." There's a variety of motivating factors involved in using particular drugs, and ignoring those is what leads to things like Prohibition, The War on Drugs, and other related failures.
If you want to stop people from doing something, you need to look at their motivations for doing it.
A related-ish thing I remember reading about is how doctors would ask folks complaining about back pain what career they were in. The goal is that folks who complain about back pain who are unemployed due to the local mill closing would get shunted into disability, while knowledge workers wouldn't.
So there's likely a pretty big effect of society telling folks that they have to be "disabled" in order for us to support them, and one way to be "disabled" is to have debilitating pain, and so you wind up with a bunch of folks who can't work and have a pain pill prescription.
It helps to separate out several aspects of the demand side:
- Addiction: may or may not be a problem at all, heroin isn't actually very expensive so the government can just keep giving it even to large numbers of people
- Other health risks: the risk of catching Hep C or dying of an overdose.
- Acquisitive crime: largely caused by the drugs being illegal.
- Morality: drug users are "bad people" because they lack moral strength or whatever. (Personally I have no truck with this, but it seems to be very important for a lot of people)
I'm not sure anyone really knows why the demand is so huge.
Unemployment seems obvious, but it's not. New Hampshire, for example, if often cited as one of the areas hit the worst by opiate addiction. Yet, it's doing well with unemployment, in relative terms.
There was a tremendous amount of unemployment during the Great Depression - far worse than now. Sure, opioids weren't as available, so people didn't turn to them. (Alcohol, on the other hand...)
But I think a lot of what people did then was turn to each other. They had deeper relationships with people than (many) people do today. Sure, you've got two hundred Facebook friends. How many of them can you call at 3 AM because your marriage is about to fall apart, or because you're feeling suicidal? Technology has given us more relationships, but I think that in the process, we've lost much of the depth. That leaves a huge hole, because people are wired to connect to people. We crave human contact, and we get tweets. It's not enough.
So my suspicion is that we're turning to opioids to try to fill that void. But as I said, this is just my suspicion.
I don't know, I see young people taking to each other about suicidal thoughts and making support groups do each other all the time. Teenagers making Discord chats where they can talk about how their families are abusive and they want to kill themselves, Skype chats where young adults discuss obscure chronic illnesses that the rest of the world can't empathize with them for.
Fair enough. Technology allows people to connect who would not have been able to in the past. But I still claim that, for the average (or perhaps median) person, the net result has been dehumanizing - it has resulted in less depth of relationship.
American doctors follow national guidelines, because if they don't they expose themselves to malpractice suits. The guidelines currently say that if someone is in pain, give them as much painkiller as they want. Their ability to use their extensive training and judgement to make a better call is somewhat limited.
> The guidelines currently say that if someone is in pain, give them as much painkiller as they want
Can you point me to those guidelines please? I'm struggling to find them.
I can understand the advice if it's relating to short term immediate pain - for example post-operative pain. Addiction is unlikely to result from pain medication use in that example.
I went looking for you. The guidelines appear to have been updated since last I checked, and are no longer as irresponsible as I thought they were. Here's what I found:
It's actually pretty hard for legitimate patients to get opioids in many circumstances. My mother has chronic pain from a surgery and has been on a very low dose of oxycodone for years now (10mg a day, I think), and she regularly is subjected to urine and other tests to prove that she's not an addict. My grandpa just had an operation and later at home ended up in a lot of pain, but he could not get oxycodone for two days -- the first night because he went in after 7:00 PM and apparently Indiana has some law against prescribing them past that time.
Huh, I might be basing my perception on what is high vs. low from knowing some people who abused oxycodone. I believe my mom takes 5mg twice a day, and from what I'm reading that still seems pretty light. Oxycontin pills are minimum 5mg, correct?
Erowid puts that in the "light" category for users with some tolerance, FWIW:
I'll have to take your word that the guidelines say effectively to give the patient what they want, it seems a strange idea.
Here, in Norway, the doctor also tells the patient to take as much as they need but the decision on the actual type of pain relief is arrived at collaboratively between the patient and the doctor, sometimes including a short stay, two or three nights, in hospital so that multiple regimes can be quickly tried out under supervision.
In some cases they can prescribe more suitable drugs and more suitable delivery methods.
For instance the pain associated with cancer is often better controlled with a Fentanyl continuous delivery patch than an Oxy capsule. Oxy is good for relatively quick relief when you have a temporary increase in pain but the effect wears off so you get uneven pain relief.
I'm not a doctor, just speaking from personal knowledge of someone very close to me.
I've heard Drew Pinsky rail against physicians for their role in the epidemic. But he also mentions an assist from the legal community in that they've taught patients they are entitled to lengthy doses of opioids.
Despite the evidence showing only short term benefits to opioid treatment physicians fear being sued by patients for refusing to continue prescriptions. I believe the argument is "Pain is the fifth vital sign."
There has to be a some kind of change in lifestyle. Like you said, trying to cutoff supply will only criminalize the activity and make it worse. I've heard, among other solutions, recommending yoga, physical therapy etc. instead of immediately prescribing opiod painkillers. This is certainly an important problem and I'm as interested as you are in what the solutions might be.
I'm going to comment here with a plug for the March For Science, on April 22.
Why?
Because the opioid epidemic started with a simple matter of scientists not being allowed to science.
Purdue Pharmaceuticals marketed oxycontin as a drug that lasts for 12 hours.
The evidence indicated it only lasted for 8.
If Purdue's scientists were allowed to act on the evidence, i.e. to be actual scientists, the whole world would have known this years ago. People prescribed oxycontin would have been told to plan for 8 hours of relief, not 12.
Instead, hundreds of thousands of patients were subjected to 4 hours of pain a day, and they sought relief with other drugs, including illegal ones. And the epidemic began.
You forgot the best part: It made Purdue rich. Instead of changing the frequency of doses, they told doctors to up the strength which made the company more money. The owners of Purdue are billionaires now: http://www.latimes.com/projects/oxycontin-part1/
> Instead, hundreds of thousands of patients were subjected to 4 hours of pain a day, and they sought relief with other drugs, including illegal ones. And the epidemic began.
No, I believe the purpose of this scheme was to let the drug wear off before the next dose, in order to reinforce the withdrawal/pain->relief cycle. Oxycodone users typically didn't seek out illegal drugs (heroin) until several years after starting prescription usage.
I totally agree with the spirit of your argument, but I think you're somewhat overstating the significance of the marketing/data mismatch here. You can't simply point to that and say "thus the epidemic began". There's a whole nexus of contributing factors at play: overprescription, socio-economic malaise, the ready availability of black market opioids, etc.
Maintenance treatments with long-acting opioids like methadone tend to come with a withdrawal that lasts for months.
Meanwhile, short-acting opiates like heroin have a withdrawal period that lasts about a week. Is it any wonder methadone patients switch back to heroin when they try to quit for good?
Mark my words, this isn't going away or getting any better. You can prosecute doctors, regulate all you want, burn fields of poppies. None of it will affect the demand nor the supply. You can't price or regulate someone out of an addiction.
If people get cut off wholesale from their prescriptions because doctors are being prosecuted for prescribing pain medication, they'll turn to heroin. Which will be available, regardless of all the opium seized, regardless of cartels dismantled.
Just like when Oxycontin went under a formulation change making it resistant to abuse, which also caused the price to spike to a dollar per milligram.
People turned to heroin because it was cheaper, more potent, and much more widely available than pharmaceuticals could ever be.
If you think pill junkies are bad, wait until you look down an alley to see a heroin junkie injecting another junkie in the jugular because all her veins are blown out. Watch your step, though, lest you get a syringe in your foot.
I've gone ahead and edited my comment, not because of your comment, but just because I felt like I wasn't making a clear point. Kratom is not even mentioned anymore, sorry.
While kratom is habit forming and can "fuck you up" if you have no tolerance, the true value is for the person already addicted to opiates looking to get clean.
If you want to keep drugs out of the hands of kids, make them all legal and watch the usage numbers fall. Banning a powdered leaf, that is quite self-regulating, albeit habit-forming, is a step backwards in the quest to put out the structure fire that the opiate crises has become.
Amphetamine will be abused by college students. Alcohol will be abused by highschool kids. It's a given. The allure of stuff like cocaine, with the "what else was I lied to about, what am I missing out on" mindset goes out the window when you stop lying and start letting people make their own choices.
You can't stop all the drug abuse but the extent of use is not a given. Amphetamine use of UK students appears to be extremely rare compared to the US, its never really been a cultural thing here.
I suspect it is due to very few amphetamine drugs being prescribed, especially to children. It seems to common to hear about people selling their legitimate ADHD/ADD prescriptions to friends in the US. "Speed Paste" is the only amphetamine properly in circulation and its use is mostly restricted to the hardcore "junkie" groups, very much frowned upon from the casual drug community.
None of the above is a solution, just to note the degree to which groups will gravitate towards and use a drug is not a given. Culture and availability probably affect use massively.
I completely agree. My example wasn't exactly the best, but relatively applicable to the US nevertheless.
You raise many good points about drug use being different geographically and culturally. It's very much about availability, local drug culture, etc.
For example, the speed paste. As you said, in the UK and in other European countries amphetamine is usually amphetamine in paste form, not crystal methylamphetamine like we usually see here in the states.
Culture and availability absolutely affects use massively, a point I didn't mean to gloss over, and one I'm glad you raised.
I think identifying these differences between countries will bring governments a step closer to finding some sort of solution. Not exactly an easy one though when it comes to culture though. How do you break strong cultural associations?
There seems to be a number of (bad)role models that glorify different drugs in sub-cultures. Opiate use is glamorised from what I can tell in southern HipHop, Cannabis promoted all over the shop, Xanax frequently referred to in Hollywood.
>Alcohol will be abused by highschool kids. It's a given
But in the UK it's not even regarded as "abuse". It's perfectly normal for 15 year olds to drink alcohol with their friends. (And not against the law, if they are doing it in private.)
There may be benefits to legalizing drugs, but the idea that it will reduce usage of them is a fantasy.
It's in that strange area between normal and looked down on that depends on the class background of the observer. It is a problem, but a slowly declining one: http://www.bbc.co.uk/news/health-31452735
Cannabis is effectively legal in the UK now, but there's no evidence of a decline in use as far as I know. Certainly not a precipitous one.
I'm not sure what you mean about class background. There must be very few 15 year olds in the UK, from any class background, who haven't used alcohol. I wasn't really referring to binge drinking. My point was that the fact that it's easier for young people to legally drink alcohol in the UK than it is in the US seems to have an effect.
Ah right, I was referring to distinction between "problematic" and "non-problematic" use. People generally accept that you can have a "non-problematic" use of alcohol but not everyone accepts that for the other drugs. Although you'll still find newspaper editorials concerned about teenage drinking. And in the really regressive papers, concern about women drinking.
While cannabis simple possession is very rarely prosecuted the police are still going after grow houses. I think it would have to be legitimised (properly legal) to see a decline due to losing the "rebel" factor.
Well, maybe. I don't think smoking cannabis is really seen as rebellious these days, though.
I don't see any reason to believe that legalizing a drug will stop people using it, or cause them to use it more responsibly than they do currently. We have a case study in the form of prohibition in the US. There's certainly no evidence that alcohol use declined following the repeal of prohibition.
Yeah, it's all over. Prescription stimulants get diverted, resold at a markup, etc.
The demand is high and the supply is there. Low doses of oral methamphetamine arent entirely uncommon either. Meth is cheaper, more potent and more widely available.
The extent to which this can be said to be driven by changes in the licensing regime versus changes in the population structure can't really be determined from this data.
It sounds like someone profits from shipping opiates to the U.S.. Someone who also controls the juristriction.
Sounds ridiculous, i know.
Mhmmm. Who could it be?
So what is the answer here? Like another poster said, there's a demand problem. How do we as a society address this? I've seen a lot of mumbles about dealing with supply problems, dealing with overdose problems, but it'd be good to head the problems off at the pass before they descend into major trouble.
I should also note, this is a burgeoning problem in the Puget Sound/Seattle region. It's not just rural people dying.
Can someone knowledgeable about drug policy / sociology provide some insight in this thread?
The problem is you have a large addicted population. Helping them get off opiates is expensive and time consuming (although orders of magnitude less than the war on drugs).
Also, depending on the level of addiction that may just be no hope for some. As another commenter said, in Holland they have had legal heroin dispensaries for 30 years, with medical staff and clean rooms for injecting. The addicts can be monitored, I believe they have general health and mental health workers available as well.
The addicts get live a "normal" as possible, knowing when and where they can get their fix. The whole day is not spent worrying where the money will come from Due to this, the average age of addict has steadily rose for years and years and, as the other commenter also stated, they die off
Heroin clinics can be very helpful for that. By providing the heroin and requiring that it be used on site they take it out of the community. Nobody sees their friends using and gets offered a bit to try. Starting drug use is often a very social phenomenon, generally people are introduced to them by friends.
From a study on the Swiss clinics [0]
>*New Use Rates: Slightly lower than expected. 1) As reported in the Lancet June 3, 2006, the medicalisation of using heroin has tarnished the image of heroin and made it unattractive to young people. 2) Most new users are introduced to heroin by members of their social group and 50% of users also deal to support their habit. Therefore, with so many users/sellers in treatment, non-users have fewer opportunities to be exposed to heroin, especially in the rural areas.
This is only helpful for people starting from heroin though, the problem of people getting addicted to opioids from taking pharmaceutical drugs
[1] is an entirely different matter to address.
I think this is mostly it. There are no new drug users coming up. Those you are addicted are maintained, those who are not too far gone are helped to reduce (most at this stage probably want off and they can see how it has destroyed / is destroying their life but don't know how)
As the market is disrupted, dealers move onto other drugs as there is no profit there, so is not so easy to find any more on the illicit market.
The situation is different to the US, whose current problems seem to be mostly from over prescription of pain pills, then when that was closed the flooding of the country with heroin and fentanyl to an already addicted population.
Purely anecdotally, the US does / did seem to prescribed lots more pain meds than any other country. When I used to use drugs (recreationally) and frequent drug forums in the early 2000s pain pills were regularly mentioned by those who used drugs recreationally for parties and were mentioned the same as party drugs, whereas in Europe they did not exist (outside the heroin scene).
Now, I live in tropical South Amercia, ,where quite a few US based expats move to each year, one of the biggest problems they have is getting their medication here. A large percentage are on a huge amount of strong medication. The expats from Europe are not. I don't think the lifestyle back home was that different, I don't think US people feel pain more than others, just that the Drs prescribe lots and lots of medication. Or perhaps European Drs just under prescribe due to public health systems and not wanting to fund the medication. Or perhaps the counter, there is more profit for the US Drs to prescribe more. Whatever the cause, there is a vast difference between the two
Preventing that first time is probably the secret. It's got to be so much harder to resist once you know what you're missing. And it's not like you're rational about it and considering long term consequences when you're confronted with a second opportunity.
Unfortunately, we live in a society where it's all good, live free, don't judge, do what feels good, etc. That leads to things that feel extremely good...
I'm grateful to parents, teachers and some scary videos in high school health class that taught me to stay away.
Not at all. The first time you use heroin it is nothing special. If it is strong, you will vomit, a lot.
The high isn't even that great. If you are in pain when you take it, then sure. If you are dope sick from other opiates, then sure.
Addition to opiates doesn't happen from that first hit, it takes effort and dedication. You need to be using multiple times, daily for over a week before you'll get sick and even then it won't be so bad.
I remember reading somewhere about how a decent chunk of drug users just plain grow out of it as they grow into life roles that it doesn't quite work for.
Nothing to do with theoretical long term consequences, just "this is more trouble than it's worth".
I'd concur.... anecdotes from reading Reddit suggest that's true for a number of pot or hallucinogen users. They move on to more fulfilling roles in life.
Well sure, for the safest, least-addictive drugs around. For more dangerous drugs like alcohol or the ones discussed in this thread, "growing out of" an abuse habit is orders of magnitude more difficult.
While there may be some truth to this, it's also reflective of our society in general - more absent parents/latch key kids, issues with access to mental health care/health care in general, a lack of jobs/hope in deprived areas, a generation of soldiers coming back from the Global War on Terror (how many homeless people are veterans?), and the many side effects of the War on Drugs - the flawed criminal justice system, deeply entrenched gangs in some areas, and the foreign policy failings in Central/South America.
It attributed addiction to living conditions (e.g. rats in "Rat Park" had less addicts than rats in laboratory cages) rather than addictive properties of the drug.
For humans, I think it goes beyond physical living conditions, and into the mental realm.
A perhaps related topic is Attachment Theory [2] which models interpersonal relationships imprinted on children by primary caregivers.
With the two income trap shunting child rearing to daycares and schools, the theory would predict less secure attachments in children, leading to various maladies including identity crises and drug abuse.
I'm familiar with both. Generally I don't think either of the conclusions/theories they establish are supported by history and the breadth of human culture, even today. Attachment theory is particularly notorious for being misunderstood.
We have ~400 overdoses per month here. ~20% of that is fatal overdoses because those ODs are from users doing it by themselves and not inside one of the shooting galleries we have set up. The safe injection sites work as advertised but for many reasons some addicts don't go there, mainly because debt collecting gangsters and drug dealers hover all around the front doors, and stigma of standing in an addict lineup that spreads for blocks for all to see.
There's a few reports here from VANDU a group run by addicts on the effectiveness of peer-run supervised injection sites and needle exchanges, meaning run by other addicts instead of government employees http://www.vandu.org/reports/
The problem is synthetic opioid is being used to buff out heroin so street dealers can save money by importing less heroin from India (how it comes into Canada). They keep coming up with new synthetics to bypass precursor prohibition or import laws, plus China has factories pumping this shit out legally which can easily be smuggled since it costs far less than heroin from India/Afghanistan.
Whenever you talk to a street addict basically the reason they got on heroin was they had some other substance abuse problem, usually cocaine, alcohol or meth, there was a shortage of that substance because either they couldn't afford it, busts made it scarce, or they were in jail so through peers they accessed heroin instead and got hooked.
Methadone doesn't work, they've already abandoned that idea here and moved to just handing out heroin to the worst cases, or hydromorphone which has a proven success rate in weening addicts off drugs.
Somewhere in all this is a solution that doesn't involve enabling career bums who want free heroin for life and doesn't involve 400+ ambulance calls per month draining our resources.
>Legal Heroin Prescriptions: The ‘British System’ You Never Knew Existed
Basically prescribe heroin for the addicts so they don't need to deal / steal and the thing dies out. You could link getting the prescription to doing something useful work wise if you want to be moralistic. Been done since the 1920s - tried and tested.
How does the "British system" work out long-term, for the addicts as individuals -- resistance accumulation, vein damage, constipation? Do any live on to old age? Or does it "work" for the rest of society because they die peacefully, at home?
There is an issue that people get 'parked' on methadone and never fully come off it. However, some people I know are now in their 70's and still managing their addiction via Methadone prescribed by a GP. They have been on this treatment since the late 80's. They would not be alive and working, paying their taxes if this wasn't about.
I'm not sure but I believe prescribed heroin has limited side effects and is fairly safe and many come off it eventually and live to an old age. I've not seen the data though.
In the UK it appears that there's a Spice epidemic. It's often called "synthetic cannabis" or "(formerly) legal highs", but it in reality it's all kinds of research chemicals sprayed onto leaves to be smoked. It has some pretty hideous side effects, and seems very addictive (https://video.vice.com/en_uk/video/the-hard-lives-of-britain...)
Oh, and the government just handed the whole market over to illegal drug dealers, with fairly predictable results.
I don't have figures so this is pure anecdote, but I was wandering around Watford last weekend and seeing people who looked like they were in the VICE documentary I linked to above.
But yes, you're of course right that our whole approach is wrong.
Spice is in some ways worse, as many U.K. prisons are reporting troubles with contraband use getting prisoners and guards alike high with secondhand smoke.
I'm on the gulf coast, and we just had a high-profile prosecution of a doctor running a pill mill.
What if this whole mess isn't so much a technical problem to be solved as much as it is our system functioning under its own perverse incentives? Other countries don't have this problem.
In my own area of expertise, I have seen so many non-solutions force-fed to the customer when an actual solution is not as profitable. It is not hard to believe that medicine operates similarly.
> What if this whole mess isn't so much a technical problem to be solved as much as it is our system functioning under its own perverse incentives? Other countries don't have this problem.
That description could easily be applied to many aspects of the US healthcare system - an epidemic is a failing of public health.
The first time I saw a TV commercial here in the US for a pill to battle opiod induced constipation, I realized just how many people are taking large doses of the stuff. Pretty staggering to me.
Yeah, those commercials are painful. If you're taking so many opioids that you have trouble pooping, maybe the solution is to take fewer opioids rather than adding another medication to the mix. Really damning commentary on how easily and flippantly we overmedicate.
So get some extra fiber and pop a Colace if it's really bad. Adding another prescription medication seems like a pound worth of solution for an ounce's worth of problem.
My Dad was prescribed tramadol for arthritis pain. Apparently tramadol is the entry level opioid. He reported to me zero relief from the pain and "poop like bricks". He doesn't want to take any more.
I've encouraged both parents to try legal marijuana products in their state before experimenting more with anything opioid related.
I'll never understand locking people up for having an addiction and treating them like criminals. I'm not too educated on how it's handled in America but in Australia you can go to your doctors and get signed up to a methadone program without worrying about any legal repercussions.
My fiancé works at a pharmacy in Melbourne, Australia and says some of the most lovely and friendly people who just want to get themselves together come in regularly to get their $5 dose and it's saddening to see how badly society judges them.
I believe you can do the same here, but the (huge, purpose-defeating) difference is that you need to be able to afford the rehab in a country that isn't so keen on providing a safety net (somewhere upthread someone mentions his sister ruining her life with heroin, wanting to go to rehab, but unable to afford the cost, which is uncovered by Medi-Cal).
I know the United States will never do it, but Singapore barely has a drug problem because they execute dealers and have mandatory treatment for users. I'm not advocating the ridiculous policy that the Phillipines has, but Singapore doesn't mess around if they find distribution levels of illegal drugs on you. There also needs to be much stricter control of new prescriptions for opioids, which lead to addiction.
>There also needs to be much stricter control of new prescriptions for opioids
Like the extremely strict controls in place? Like the prosecution of doctors who run pill mills? Like the rescheduling of hydrocodone formulations?
In my local ER there is an entire framed info-poster explaining why you aren't getting your meds refilled at the ER, you won't be getting fentanyl, dilaudid or oxycodone prescribed to you no matter what. ED's work with your primary care doctor and relay info to them. States have implemented pharmacy tech that allows them to track prescriptions state-wide. (a former massive problem)
Hospitals are already doing this. Pharmacies, already doing this. Doctors are terrified of the laymen telling them they know better in the court of law. Pain is being undertreated now more than ever, which is the flipside to the crackdown you don't seem aware of, which has been happening for years now.
There will always be abusers. It's inevitable. The people who really suffer from this kind of over-reach are people like my grandparents who are nearing life's end. People dependent on pain medication for their quality of life. Non-abusers.
Maybe quality of life means nothing to you, but to them it's all they have left keeping them going. It's the only reason they can continue to live through the constant pain, the enduring misery old age and lives of very hard work has wrought upon them.
Experts have been questioning Singapore numbers for a while now. They are probably not that low and theres plenty of evidence of drug use in the country:
On top of that, how come other countries that have strict drug regulations and intensive prosecution (for example, Thailand) don't show same low rates of consumption?
Singapore is a very small and extremely centralized city-state. America is an enormous country with a long history of decentralized governments. I imagine very few dealers or addicts can slip the net in such a small place, not so much for America, perhaps.
And all of that relies on the assumption that Singapore's way is the best method that we as a culture (and to a greater degree as a species) can hope to accomplish. In my opinion, Singapore's drug policy is lacking in nuance.
The U.S. tried very harsh punishment to stop drug use, the War on Drugs. It resulted in massive increases in incarceration; millions of innocent lives ruined (along with their families' lives); massive costs to society for law enforcement, prisons, crime and violence; and not much impact on drug use.
The only thing that is good about this epidemic is that it seems to have moved harm reduction onto the agenda after decades of militarized and/or "lock 'em up and throw away the key" responses. Hopefully the result will be a more rational response for all of America's drug problems regardless of the color of the users.
Are you kidding? The attorney general of the United States is on record saying the one thing that kept him from joining the KKK was their marijuana use, stating that "decent people don't smoke marijuana."
Public opinion may have shifted, but as far as the current White House is concerned, it's their way or the highway.
For the record I've noticed the tone of reporting these days is a little different as well, personally. It is harder for people to demonize prescription drug abuse; you don't get quite as much of the broad stereotyping and Hollywood-ization that happened in the 1980s on this subject.
Yes, some people cling to old-fashioned hardened attitudes. But if you look at Gallup's poll on drugs (http://www.gallup.com/poll/1657/illegal-drugs.aspx), people are way more worried about prescription drugs and the related heroin epidemic these days. Way more than cocaine, certainly. It's not in the poll, but it's hard to remember when the last time the boogeyman of the 1980s (crack cocaine) came up in reports.
Support for marijuana legalization stands at 60% now, compared to the 1980s where support was at 25%. There is a large age gap in support, in marijuana at least (http://www.gallup.com/poll/196550/support-legal-marijuana.as... -- 55+ 45% support, 18-34 77% support).
Although I'm sure harder stances will linger onward, as it has in the AG's mind, the AG's stance is increasingly looking out of touch.
Everywhere. I don't know if you were around in the 80s and 90s but the contrast in rhetoric about drug use is amazing. Both sides of politics were tripping over themselves to be tougher on drug crime back when it was perceived as a non-white problem.
I was, and I think the penalties and number of people in "the system" for drug offenses is significantly higher than it was in the 80s and 90s. We now have more people (not percentage of people) incarcerated than any other country, even China. The rhetoric may be softer, but I don't think the judges are.
>States have since cracked down on prescription opioid abuse, creating drug-monitoring programmes and arresting unscrupulous doctors.
So if you look at the chart, when they started doing this, heroin overdoses skyrocketed while pill overdoses stayed about the same. They doubled the deaths with their crackdown solution, as if that has ever worked.
> The opioid epidemic has its roots in the explosive growth of prescription painkillers. Between 1991 and 2011, the number of opioid prescriptions (selling under brand names like Vicodin, Oxycontin, and Percocet) supplied by American retail pharmacies increased from 76m to 219m. As the number of pain pills being doled out by doctors increased, so did their potency. In 2002 one in six users took a pill more powerful than morphine. By 2012 it was one in three.
I find this absolutely outrageous. I'm not American, but I stumble upon articles mentioning this, and I do watch enough American TV series and movies to have an idea of how acute the problem is (it's crazy how often in TV series doctors seem to give pain killers like it's candy).
I have the impression that in Europe, painkillers are much less used but I would not be surprised if the American trend were to contaminate medical practice here.
Pain is a minor consequence of disease or trauma. Pain won't kill you, so why would you risk become addicted to very dangerous drugs just to relieve it?
There speaks someone young and healthy. Some conditions are extremely painful in the long term.
"It is estimated that more than 100 million people suffer from chronic pain in this country,[11] and for some of them, opioid therapy may be appropriate. The bulk of American patients who need relief from persistent, moderate-to-severe non-cancer pain have back pain conditions (approximately 38 million) or osteoarthritis (approximately 17 million)."
"aggressive marketing by pharmaceutical companies"
"United States their biggest consumer globally, accounting for almost 100 percent of the world total for hydrocodone (e.g., Vicodin) and 81 percent for oxycodone (e.g., Percocet)"
That does make it sound like a problem created by pharma drug pushing on TV. But that doesn't mean the pain isn't real either.
Really the whole thing needs to be seen as a widespread public and social health problem - which is exactly the sort of thing the US system is set up to avoid seeing. Healthcare is not just a matter of individual responsibility or a contract between someone and their employer.
> "aggressive marketing by pharmaceutical companies"
I'm wondering what that means, concretely. How exactly do they convince GPs to prescribe pain killers even when it's not really appropriate? They can't just pay them, can they?
One of the best books I've ever read on why the war on drugs is
a bad idea. It's written by a UK cop who was there nearly from the
beginning.
https://www.amazon.com/Good-Cop-Bad-War/dp/1785032690/
Good Cop, Bad War (Paperback)
Publisher: Ebury Press
Language: English
ISBN-10: 1785032690
ISBN-13: 978-1785032691
I say this mostly tongue-in-cheek because I hate to apply one bad policy to fix another, but I bet if narcotic overprescription could more readily trigger medical malpractice, you'd see doctors thinking more judiciously about their use.
What's funny is there is no evidence that these opioid pain killers are actually effective in the long term for the management of pain. If it wasn't for lobbying they likely wouldn't be legal to use in that way.
Stop taking them for a few days and you'll see what I mean. Many studies have shown that patients who do not consume opioid medications have better long term outcomes than those who do. It simply isn't effective in managing pain long term, and also is not indicated for use in that manner.
When I stop taking them I'm in pain again. I think what you're trying to get at is the opioids don't solve the underlying problem. But to say they're not effective for managing pain is wrong. I use them to manage pain every day. I get regular steroidal-epidural injections to solve the issue.
Read Chasing the Scream [1], a fantastic book that documents drug prohibition in the USA, how doctors who viewed it as a health issue got chased out of their desire to help, and suggests many paths to helping people and making the world a better, safer place.
I've posted this in enough threads that I probably seem like a bot advertising for it, but seriously, it's a book worth reading and that can change someone's entire opinion on the drug epidemic and what legislation we should pass.
Although the entire article is worth reading, jump down to the paragraph that begins with "The opioid epidemic..." and read for about ~5 paragraphs if that's all that interests you.
This is hardly news: the same dynamic played out in a different chronological order between alcohol and marijuana prohibition. Alcohol was so ubiquitous that Prohibition turned all of society (including "decent" people) into criminals, so the response was that it's clearly an unworkable solution; we can't lock up _everybody_. It's only simplifying a bit to say that marijuana shared much the same ubiquity in certain _other_ communities, so the response was.....let's just lock up everybody.
Could weed slow down the opioid epidemic? It gets you high, it is way cheaper, way healthier (not smoked), it isn't addictive, curbs the urge for opioids, easier to make, easier to sell.
These stories are so frightening to me that I contemplate just enduring the suffering if I am ever unfortunate enough to be prescribed oxy or dilaudid.
I once read of a 20-year-long study that found that when heroin-addicted UK doctors were given unlimited access to pure heroin they performed slightly better than their non-heroin-addicted colleagues, and they had no negative long-term health consequences. If anyone else has heard of this study, or especially if they have some documentation on it, I would appreciate a link.
There is something obviously wrong or at least strange with the data that backs that map. Look at the contrast across the border between Tennessee and Georgia or between West Virginia and Virginia. I think some states must be under-reporting things or reporting them differently. I would expect such a map to track poverty maps or unemployment maps, but it does not.
The states with medical cannabis don't have anywhere near this problem. They need to cover medical cannabis via medicaid that would seriously put a dent in the crisis or at least keep it from growing bigger.
I _wondered_ what the political & law enforcement community was going to do, with the clear failure of the War on Drugs and growing demands for legal marijuana.
Never fear! Here's the latest Demon Drug, which we can use to whip up popular support for another round of failed prohibition-mentality policies. No need to worry about budget cuts, reduction in the availability of military weapons, drones, etc. to law enforcement. There will still be a viable career in persecuting some of the most vulnerable members of society.
Those in favour of harm minimisation need to fight for legalisation, or at the very least decriminalisation as a strating point. Not just for _their_ favourite drug, but for those causing the most harm right now.
One side effect is that people who are using drugs responsibly are executed when they forget to empty their bags on the way home.
A friend of mine from Singapore had this happen to her friend.
Being completely draconian is not a solution to anything. We can fine people 100K for parking illegally, and you might get fewer people parking badly, but it will never seem to be reasonable.
Hard to believe there is really an "epidemic" beyond typical fearmongering and political noise. People have always used drugs, this is nothing new. Unfortunately all the hype and noise is having significantly negative consequences to the medical community, doctors, and patients who actually need these things.
I offer links to an engaging blog post [0] and a scholarly paper [1] that both suggest there is more to the epidemic than 'fearmongering and political noise'. Could you elaborate on the evidence for your beliefs?
It's a "national health crisis" because of the ethnicity and locations of the people it's affecting. Today, politicians are proposing more treatments and going after the pharmaceutical companies[1]. Back in the 80's and 90's, the response to the crack epidemic was harsher prison sentences for users and sellers because it was largely minorities who were affected[2].
Not arguing that treatments shouldn't be made available but it's important to keep all this in mind if someone ever suggests that all are equal in the eyes of the law when it comes to drug offenses.
Epidemic may be a strong word, but the rate of opiate overdose deaths certainly does seem to be increasing, and it's likely that cracking down on the supply of pain pills is a contributing factor to this.
'People have always done x' is the stupidest response possible to this sort of problem. Of course people have always done drugs, but the RATIO of people doing them to not fluctuates. There is a huge difference between 1% of the people doing opiates and 100% of the people, and to act like there isn't is disingenuous and dangerous.
I'm from those plains and my guess is folks there refuse such drugs, even when they may need them (like after surgery), because:
1. They're tough people. A little pain means you're still alive!
2. They don't want to get hooked - too many people/animals rely on them.
3. Social stigma associated with such drugs.
I had foot surgery a couple of years ago and the Dr. tried to prescribe me opioids but I refused. I've seen the damage getting hooked on those can cause (in Dallas) and don't want that junk anywhere near my life.
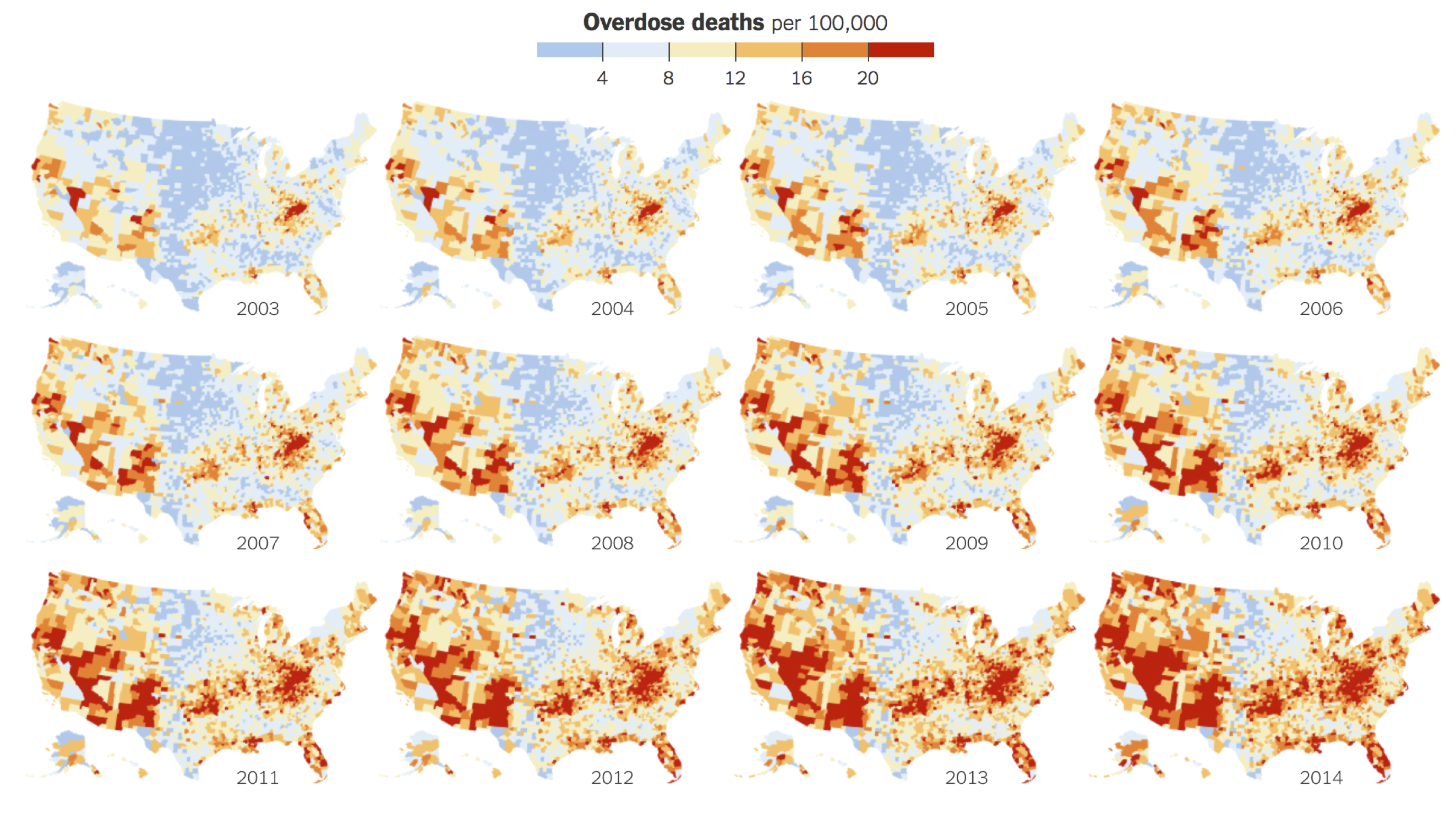{kind=link}
There were recently two shootings within a mile of my house. Several people dead. Both shootings were drug related.
I can't help but look around and believe that the needs these folks are trying to satisfy are completely human, and that forcing the users to resort to black markets leads to violence and overdoses. I can't help but think this problem in my community could be solved by simply letting people get high.
Maybe the answer isn't to make heroin available OTC at Walgreens, but supervised injection sites seem to be gaining traction[1]. I think a lot of the dark red spots on the map, like mine, should probably consider this option.
It's not like anything else is working.
[0]http://www.tribtoday.com/news/latest-news/2017/03/fri-920-pm... [1]http://www.seattletimes.com/seattle-news/health/safe-injecti...